Anatomical Context: The Meninges
Understanding ICH subtypes requires knowledge of the brain's protective layers, called the meninges. From outermost to innermost:
- Skull (Calvarium): The hard bone protecting the brain
- Dura Mater: Tough, outermost meningeal layer attached to the skull
- Arachnoid Mater: Middle layer forming a web-like structure
- Subarachnoid Space: Space containing cerebrospinal fluid and blood vessels
- Pia Mater: Thin innermost layer adhering to brain surface
- Brain Parenchyma: The brain tissue itself
- Ventricular System: Interconnected cavities containing cerebrospinal fluid
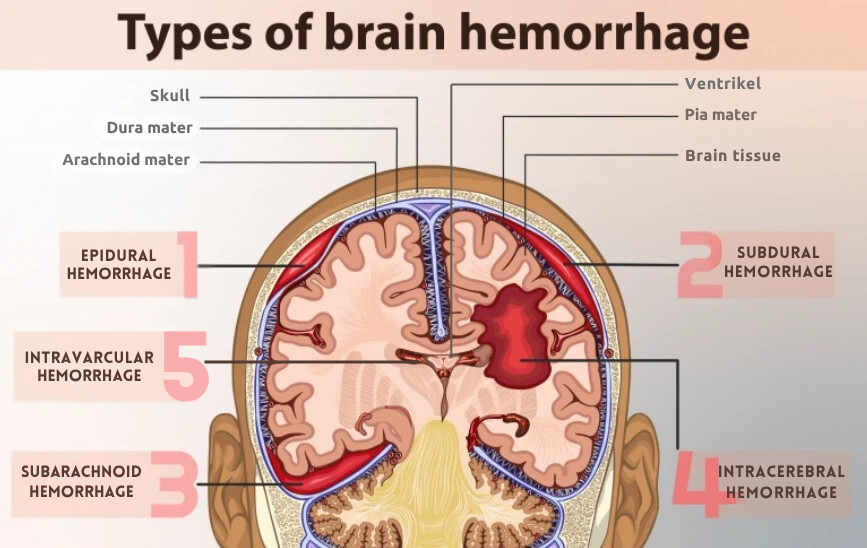
Diagram showing layers from skull to brain tissue with ICH locations